#MS Research how does NIce measure value for money
How NICE measures value for money in relation to public health interventions
How NICE measures value for money in relation to public health interventions
Is the National Institute of Clinical Excellence really NICE and an look after the financial purse. Yesterday ProfG was attacked for his views about what is included and what is not.
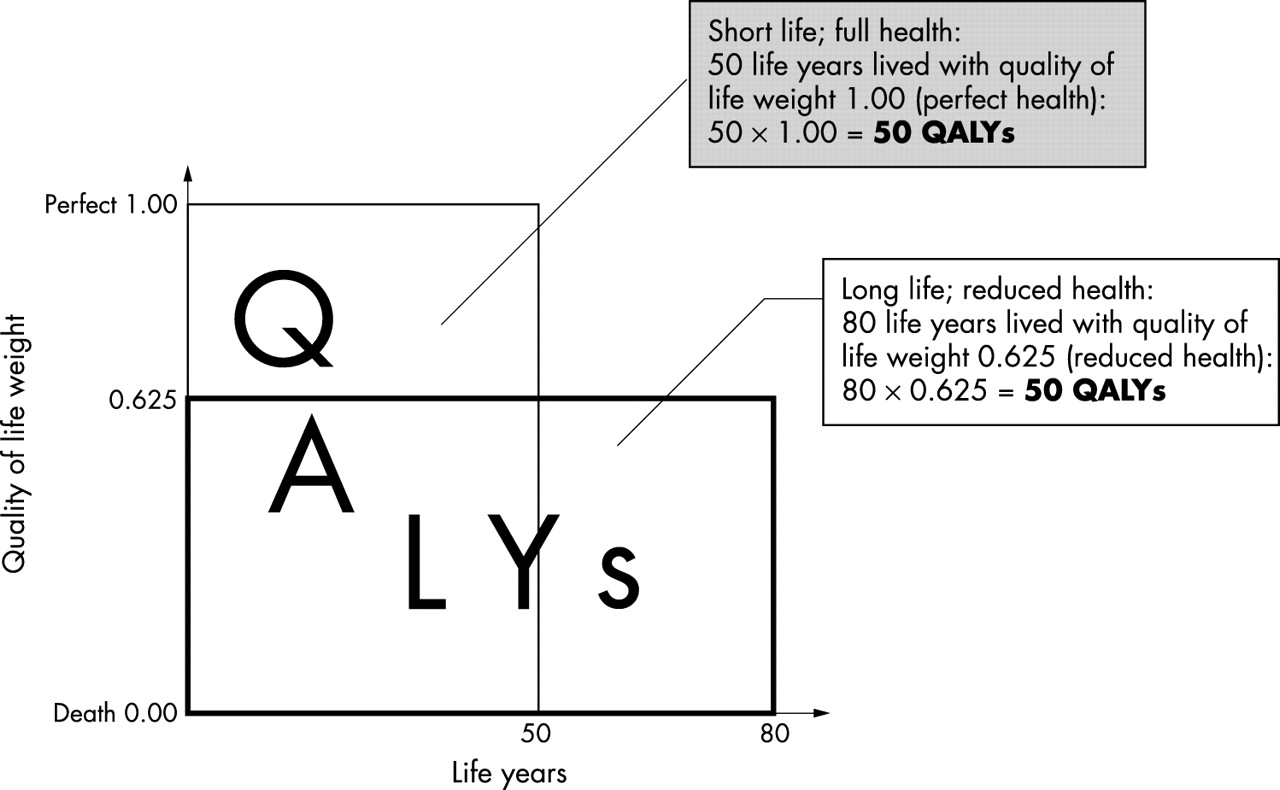
Cost–utility analysis considers people's quality of life and the length of life they will gain as a result of an intervention. The health benefits are expressed as quality-adjusted life years(QALYs).
Generally, NICE consider that interventions costing the NHS less than £20,000 per QALY gained are cost effective. Those costing between £20,000 and £30,000 per QALY gained may also be deemed cost effective, if certain conditions are satisfied. There may be other significant benefits that are not captured by the QALY.
So at US costs then no current DMT would pass this test, so this is why we there are price negotiations between pharma and the NHS,
but it means you do not have the choice and it takes so much longer to get access to drugs.
The reports says Cost–consequences analysis considers all the health and non-health benefits of an intervention across different sectors and reports them in a disaggregated form
The following costs can be included:
Direct costs, including for health care, social services and transportation
Indirect costs, including productivity losses and for criminal justice expenditure
Intangible costs, including those related to quality-of-life and the impact of living with pain.
All impacts and costs are considered (even if the impacts cannot be costed) when deciding which interventions represent the best value. This distinguishes it from cost–benefit analysis. May not provide a good measure of value for money and would not be used as the sole basis for decisions.
Is this something new and NICE have changed the rules from when the Risk Sharing Scheme was set up? I thought it was cost of drugs only?
Do You agree? Does Prof G agree?
Pharma are out to make a buck and will take whatever they can get. What we clearly need are some cheap alternatives and then the need for NICE disappears. Is that possible?