Wouldn't it be a tragedy if we show in 100 years that repleting the population of vD prevented a large proportion of MS? #MSBlog #MSResearch
Sun-blockers: It is well known that over the last 15-20 years dermatologists and the cosmetic industry have massively increased our consumption of sun blockers. Dermatologists tell us to avoid sunburn to prevent skin cancer and the cosmetic industry to prevent sun damage that is a major cause of skin aging. Sun blockers reduce the skin's production of vD and are clearly contributing to the rising incidence of vD deficiency? Men be warned the cosmetic industry are targeting you; there is an ever increasing consumption of cosmetics with sun-blockers by men, in particular the younger generation. Almost all of the new male cosmetics now include sun blockers badged as anti-aging agents.
Outdoor activities: Other behavioural changes has been the shift from outdoor activities to indoor activities. Children and teenagers now spend much less time in the sun. Why? This is the era of facebook and gaming. Young girls spend large amounts of time on social networks and boys playing computer games. There are several studies from the past that have demonstrated that outdoor activities in childhood protect against MS; reversing this trend is very worrying.
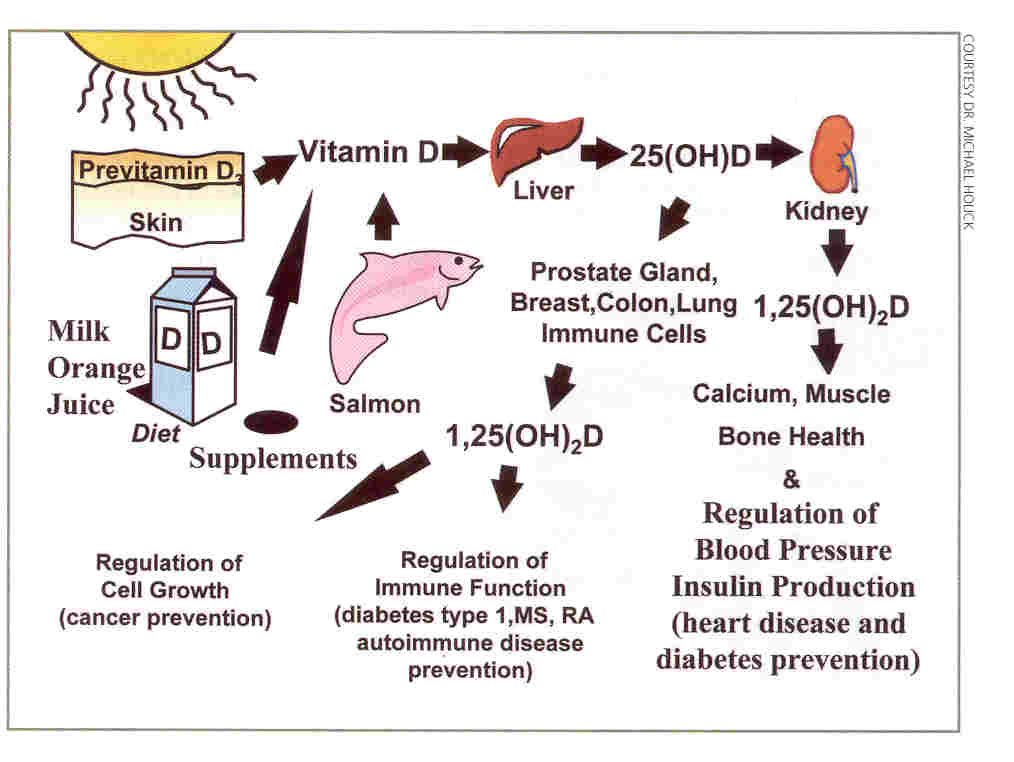
Fish consumption: It is well known that fish consumption worldwide is going down. This is based on economic factors, as we deplete fish stocks prices have risen and consumption has dropped. We are also increasingly eating farmed fish which has about a third of the vD levels of wild fish; wild fish have higher vD levels because of their diet is higher in phytoplankton which provides the vD.
Pollution and weather: Atmospheric pollution and cloud cover is another issue; this is a particular problem in certain areas of the world. In heavily polluted areas of the world air pollution exacerbates vD deficiency as it acts a ultraviolet B light filter.
Cultural changes: I have mentioned before that covering up for cultural reasons is a problem for woman. Whether or not covering up is for religious or other cultural reasons it contributes to very low vD levels in some parts of the world.
Outdoor activities: Other behavioural changes has been the shift from outdoor activities to indoor activities. Children and teenagers now spend much less time in the sun. Why? This is the era of facebook and gaming. Young girls spend large amounts of time on social networks and boys playing computer games. There are several studies from the past that have demonstrated that outdoor activities in childhood protect against MS; reversing this trend is very worrying.
Fish consumption: It is well known that fish consumption worldwide is going down. This is based on economic factors, as we deplete fish stocks prices have risen and consumption has dropped. We are also increasingly eating farmed fish which has about a third of the vD levels of wild fish; wild fish have higher vD levels because of their diet is higher in phytoplankton which provides the vD.
Pollution and weather: Atmospheric pollution and cloud cover is another issue; this is a particular problem in certain areas of the world. In heavily polluted areas of the world air pollution exacerbates vD deficiency as it acts a ultraviolet B light filter.
Cultural changes: I have mentioned before that covering up for cultural reasons is a problem for woman. Whether or not covering up is for religious or other cultural reasons it contributes to very low vD levels in some parts of the world.
Low vD recommended daily allowance (RDA): The current RDA of vD of 400IU per day is based on rickets prevention studies in the early half of the 20th century. When these studies were done the role of vD in immune and other functions were not known. There is an international lobby that is trying to get the RDA of vD increased; however, without more data it looks as if public health doctors are reluctant to adopt the advice. We now promote physiological vD supplementation in all children and relatives of MSers as per the Vitamin D Council's recommendations. Despite this we have found that adherence to our advice is poor. Therefore we have started Digesting Science. This is a course to teach children of MSers about MS and the link between low vD and MS. The idea is to get children to be adherent to their vD supplementation regimen via education. "
Huang et al. Surge in U.S. Outpatient Vitamin D Deficiency Diagnoses. National Ambulatory Medical Care Survey Analysis. South Med J. 2014 Apr; 107 (4) :214-7.
OBJECTIVES: In light of the growing medical interest in the potential consequences of vitamin D deficiency, it is important that clinicians are informed about the varying factors that may complicate the assessment of vitamin D status and the diagnosis of deficiency. To better understand the frequency of vitamin D deficiency diagnoses in the ambulatory setting over time, the objective of this investigation was to examine unspecific, general, and bone-related vitamin D deficiency diagnoses between 2007 and 2010 and to determine whether the rate ofdiagnoses differed by patient age and sex.
METHODS: We used data from the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey to assess the rate of vitamin D deficiency diagnoses provided between 2007 and 2010 during outpatient visits with non-federally employed physicians in offices and hospitals. Two hundred ninety-two unweighted patient visit records were included. Trends in vitamin D deficiency diagnosis over time, diagnosis of bone disease associated with a vitamin D deficiency diagnosis, and patient age and sex were reported.
RESULTS: The number of diagnoses for vitamin D deficiency rapidly increased from 2007 to 2010. More than 97% of diagnoses were for unspecific vitamin D deficiency; 9.6% of vitamin D deficiency visits also resulted in a diagnosis of osteoporosis or bone fracture.
CONCLUSIONS: Although the rate of diagnoses for vitamin D deficiency increased between 2007 and 2010, many diagnoses rendered were for nonspecific disease; therefore, vitamin D deficiency screening may have been ordered for preventive care purposes rather than as a diagnostic aid.
OBJECTIVES: In light of the growing medical interest in the potential consequences of vitamin D deficiency, it is important that clinicians are informed about the varying factors that may complicate the assessment of vitamin D status and the diagnosis of deficiency. To better understand the frequency of vitamin D deficiency diagnoses in the ambulatory setting over time, the objective of this investigation was to examine unspecific, general, and bone-related vitamin D deficiency diagnoses between 2007 and 2010 and to determine whether the rate ofdiagnoses differed by patient age and sex.
METHODS: We used data from the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey to assess the rate of vitamin D deficiency diagnoses provided between 2007 and 2010 during outpatient visits with non-federally employed physicians in offices and hospitals. Two hundred ninety-two unweighted patient visit records were included. Trends in vitamin D deficiency diagnosis over time, diagnosis of bone disease associated with a vitamin D deficiency diagnosis, and patient age and sex were reported.
RESULTS: The number of diagnoses for vitamin D deficiency rapidly increased from 2007 to 2010. More than 97% of diagnoses were for unspecific vitamin D deficiency; 9.6% of vitamin D deficiency visits also resulted in a diagnosis of osteoporosis or bone fracture.
CONCLUSIONS: Although the rate of diagnoses for vitamin D deficiency increased between 2007 and 2010, many diagnoses rendered were for nonspecific disease; therefore, vitamin D deficiency screening may have been ordered for preventive care purposes rather than as a diagnostic aid.