Yesterday I caused a bit of
concern by a post on myelination as a GABA (inhibitory nerve transmitter) blocker
stimulated developmental myelination, so people were worried about their GABA receptor
stimulating drugs. Would they block repair? Answer is I do not definitively know
but suspect not.
In contrast there could be implications that stimulation of GABA could save nerves. Again we don't have the data.
I will try explain a bit, but it
is very, very complicated.
First things first, the report of GABAergic control of myelination is based on developmental myelination
(myelinating nerves from the first time), and as the docs from Cambridge/Edinburgh
have shown remyelination may not be the same process as developmental
myelination.
Next it is far more complex than
just GABA. What else has to be stimulated?
We have already been told that
the oligodendrocyte precursor cells get stimulated by glutamate (excitatory
nerve transmitter). This transmits their function via activity on glutamate receptors. Here there are lots of types, over twenty receptor genes. There are three main ionotrophic (opens channels for electrically charged (ion) sodium calcium or potassium) subtypes
AMPA, Kainate and NMDA binding subtypes
Myelination first acts via the
AMPA sensitive variants, then their influence stops whilst the NMDA-sensitive subtypes
come into play. This process will be influenced by the GABA receptors. This
stimulates developmental maturation of the oligodendrocyte precursor cell and
myelination of un-myelinated nerves. During this process the glutamate
receptors and ion channels get down regulated. It is not the odd one, but loads
of them.


Next there are more than one type
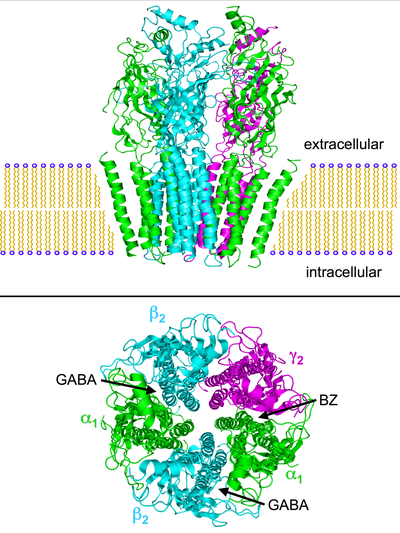
of GABA receptor. There are two main types. One is GABA A and the other is GABAB. GABA A is an ionotrophic (via chloride) channel that can be stimulated by
different types of drug as it has multiple sites and there are multiple genes making a multi-component receptor.

GABA B is a metabotrophic receptor which G protein coupled receptor that is
linked signalling to control calcium channel activity and can signal via potassium
channels.
Baclofen is the main GABA B
receptor stimulator, used for spasticity. GABApentin, Pregabalin look like GABA
but do not bind to the GABA receptors, although they may influence GABA
production they act via ion channels to be anti-convulsants and pain
controllers. The story about GABA and oligodendrocytes involved GABA A receptors, so the story is not about these drugs
Any drug used in humans would never block the GABA A receptor to the extent used in the experiments so a block would never happen in humans. Experimental studies often use crazy doses of drugs to show a theorhectic possibility or define a mechanism. But they have no translational value.
If the authors had read the ARRIVE guidelines about reporting experimental studies, they could have talked about the translatable aspects and if they had used clinical concentrations of GABA A blocking drugs, I bet they would have shown nothing...Nothing does not make for a good publication. But until this expriment is done, no cause for concern.
The importance of this post was to show that oligodendrocytes have ionotrophic function and they have loads of ion channels including loads of potassium channels.