Genetic, Immune-Inflammatory, and Oxidative Stress Biomarkers as Predictors for Disability and Disease Progression in Multiple Sclerosis.
Kallaur AP, Reiche EM, Oliveira SR, Simão AN, Pereira WL, Alfieri DF, Flauzino T, Proença CM, Lozovoy MA, Kaimen-Maciel DR, Maes M.Mol Neurobiol. 2016 Jan 5. [Epub ahead of print]
The aim of this study was to evaluate the TNFβ NcoI polymorphism (rs909253) and immune-inflammatory, oxidative, and nitrosative stress (IO&NS) biomarkers as predictors of disease progression in multiple sclerosis (MS). We included 212 MS patients (150 female, 62 male, mean (±standard deviation (SD)) age = 42.7 ± 13.8 years) and 249 healthy controls (177 female, 72 male, 36.8 ± 11 years). The disability was measured the Expanded Disability Status Scale (EDSS) in 2006 and 2011. We determined the TNFβ NcoI polymorphism and serum levels of interleukin (IL)-6, tumor necrosis factor (TNF)-α, interferon (IFN)-γ, IL-4, IL-10, and IL-17, albumin, ferritin, and plasma levels of lipid hydroperoxides (CL-LOOH), carbonyl protein, advanced oxidation protein products (AOPPs), nitric oxide metabolites (NOx), and total radical-trapping antioxidant parameter (TRAP). The mean EDSS (±SD) in 2006 was 1.62 ± 2.01 and in 2011 3.16 ± 2.29, and disease duration was 7.34 ± 7.0 years. IL-10, TNF-α, IFN-γ, AOPP, and NOx levels were significantly higher and IL-4 lower in MS patients with a higher 2011 EDSS scores (≥3) as compared with those with EDSS < 3. The actual increases in EDSS from 2006 to 2011 were positively associated with TNF-α and IFN-γ. Increased IFN-γ values were associated with higher pyramidal symptoms and increased IL-6 with sensitive symptoms. Increased carbonyl protein and IL-10 but lowered albumin levels predicted cerebellar symptoms. The TNFB1/B2 genotype decreased risk towards progression of pyramidal symptoms. Treatments with IFN-β and glatiramer acetate significantly reduced TNF-α but did not affect the other IO&NS biomarkers or disease progression. Taken together, IO&NS biomarkers and NcoI TNFβ genotypes predict high disability in MS and are associated with different aspects of disease progression. New drugs to treat MS should also target oxidative stress pathways.
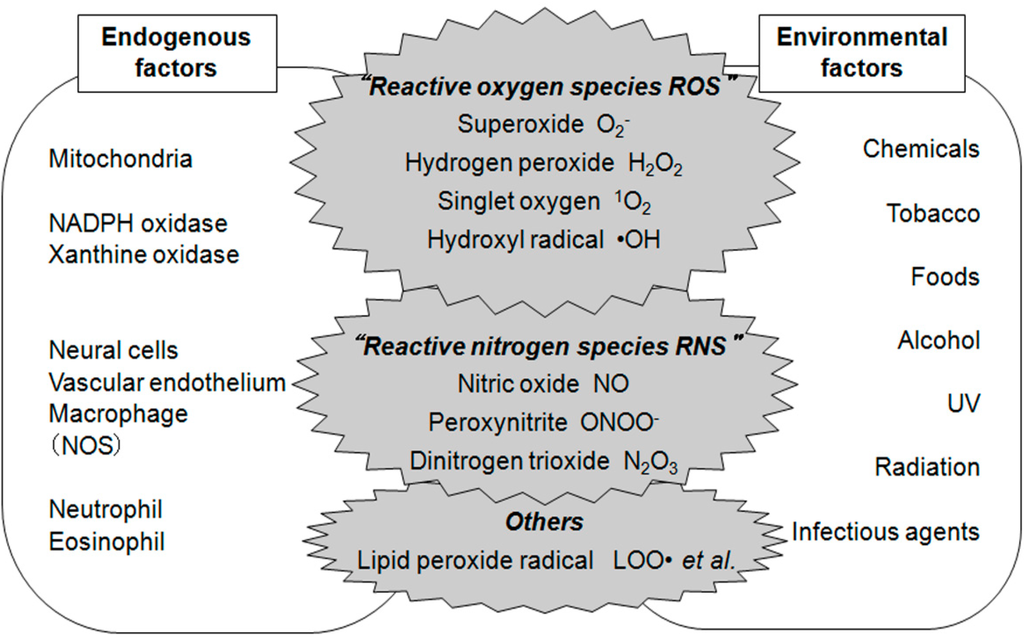
Generally, with mutations there is a change in the synthesis of the protein which may improve or lessen the activity of the said protein; and as TNFβ Ncol polymorphistm worsens disability it's possible that there is augmentation or facilitation of its action. ROS and RNS generally become a problem in neurological disorders when the levels produced exceed scavenging capacity (i.e. removal of the offending compound), which leads to cells undergoing either oxidative and/or nitrosative stresses and cell death. This process is not unique to MS but is frequently seen in stroke, as a result of ischaemia of the brain tissue, after head injury and other neurodegenerative diseases. As far as MS is concerned the understanding is that ROS and RNS are overproduced during the inflammatory activity, but lately it has also been demonstrated that mitochondrial of glial cells also generate these. None of these findings are novel on the whole.
But, why do neither IFN-β or glatiramer acetate have no effect on ROS/RNS species studied (I'm going to ignore the finding on treatment effect as the sample size and duration of the study is not long enough to demonstrate a benefit of 1st line therapy on disability)? For a biomarker study, on the other hand, 212 subjects is a moderate sample size and entirely viable to establish a trend if there is one...
So the authors go on to conclude that treatments targeting oxidative stress pathways should be considered - a nebulous statement if there was one! It's not that neither therapies have an direct/indirect effect on the pathway; because as anti-inflammatory therapies I'd say this was a given. It may be because these are not targeting the process that is overproducing this to an excess in MS. The authors do not expand further on this, but I believe the answer may lie in the mitochondria themselves...