Clin Neurol Neurosurg. 2017 Sep 7;162:80-84. doi: 10.1016/j.clineuro.2017.09.004. [Epub ahead of print]
Stereotactic radio surgery and radio frequency rhizotomy for trigeminal neuralgia in multiple sclerosis: A single institution experience.
Holland MT, Teferi N, Noeller J, Swenson A, Smith M, Buatti J, Hitchon PW.Abstract
OBJECTIVES:
For patients with medically unresponsive trigeminal neuralgia (TN), surgical options include micro vascular decompression (MVD), radiofrequency rhizotomy (RF), and stereotactic radio surgery (SRS). Multiple sclerosis (MS) is a demyelinating condition that can be associated with TN, but is not amenable to treatment with MVD. We sought to identify the outcome differences of patients with TN in MS undergoing SRS or RFR in an attempt to identify factors that may influence outcomes. We also evaluated cost outcomes, both initially and over time, based on the index procedure. We performed a retrospective review of our experience with 17 cases.
PATIENTS AND METHODS:
A single institution retrospective chart review was performed. Since 1997, 17 patients with TN and MS have been treated at our institution. All patients underwent a preoperative MRI to rule out a compressive lesion. Patients either underwent SRS (n=7) or RFR (n=10) as their index procedure and were evaluated as a group based on this first procedure. Outcome measures included preoperative Expand Disability Status Score (EDSS) scores, pre- and postoperative facial pain and medication use, post-intervention facial numbness, need for subsequent procedures, and duration of follow-up. Charges for the index procedure, subsequent interventions, and total costs were tabulated and analyzed in 2017 US dollars, adjusting for inflation.
A single institution retrospective chart review was performed. Since 1997, 17 patients with TN and MS have been treated at our institution. All patients underwent a preoperative MRI to rule out a compressive lesion. Patients either underwent SRS (n=7) or RFR (n=10) as their index procedure and were evaluated as a group based on this first procedure. Outcome measures included preoperative Expand Disability Status Score (EDSS) scores, pre- and postoperative facial pain and medication use, post-intervention facial numbness, need for subsequent procedures, and duration of follow-up. Charges for the index procedure, subsequent interventions, and total costs were tabulated and analyzed in 2017 US dollars, adjusting for inflation.
RESULTS:
The median age of patients at first operation in each group was 58.5±10.9 and 63.5±7.5 for SRS and RFR respectively. There were no significant differences in basic demographics. Overall, 71% of these patients had an excellent or good initial pain outcome. Over time, 60% of RFR and 29% of SRS patients required additional procedures to obtain satisfactory pain relief. The patients who underwent RFR as their index procedure required a significantly higher number of procedures to achieve adequate pain relief (RFR=2.7 vs SRS=2.0 [p=0.04]). The average index procedure costs in US dollars were significantly different (SRS=53,300±5257 vs RFR=12,315±3387). The average subsequent costs (costs incurred following the initial intervention) (SRS=8320±17,842, RFR=36,002±46,767) and total costs (SRS=61,620±16,087, RFR=48,317±48,475) were not statistically significantly different.
The median age of patients at first operation in each group was 58.5±10.9 and 63.5±7.5 for SRS and RFR respectively. There were no significant differences in basic demographics. Overall, 71% of these patients had an excellent or good initial pain outcome. Over time, 60% of RFR and 29% of SRS patients required additional procedures to obtain satisfactory pain relief. The patients who underwent RFR as their index procedure required a significantly higher number of procedures to achieve adequate pain relief (RFR=2.7 vs SRS=2.0 [p=0.04]). The average index procedure costs in US dollars were significantly different (SRS=53,300±5257 vs RFR=12,315±3387). The average subsequent costs (costs incurred following the initial intervention) (SRS=8320±17,842, RFR=36,002±46,767) and total costs (SRS=61,620±16,087, RFR=48,317±48,475) were not statistically significantly different.
CONCLUSION:
TN in the setting of MS is highly difficult to treat medically with SRS and RFR being offered as options for these patients. Both can provide good initial pain relief. For patients who have RFR as their initial procedure, a larger number of procedures are required for relief compared to patients who initially underwent SRS. While there is a significant difference in the cost of the initial procedure, over time, with the cost of required subsequent interventions, there is no significant difference in total costs between the two groups.
TN in the setting of MS is highly difficult to treat medically with SRS and RFR being offered as options for these patients. Both can provide good initial pain relief. For patients who have RFR as their initial procedure, a larger number of procedures are required for relief compared to patients who initially underwent SRS. While there is a significant difference in the cost of the initial procedure, over time, with the cost of required subsequent interventions, there is no significant difference in total costs between the two groups.



Figure: Trigeminal nerve involvement in MS at root entry zone (white arrow points to an MS plaque, Mills et al. The British Journal of Radiology 2010)
Whoever said "if pain must come, may it come quickly" knew nothing about trigeminal neuralgia (TN). For those of you who have not come across TN, it is characterized by swift attacks of severe stabbing facial pain (normally affecting one side of the face), occurring anywhere between a few episodes/day to more than a couple/hour. It is not uncommon to discover sufferers have had whole sections of their teeth removed in an attempt to halt the pain! Thankfully, dentists are now more aware of this disorder and know to refer to a specialist.
It is very rare in the general population (12 per 100,000), but is 20x commoner in MS. It is thought that central demyelination/MS plaques in the region of the trigeminal nerve root entry zone leads to the condition (see figure above). In a majority of cases the treatment is conservative using carbamazepine (an anti-epileptic) in the first instance, and three-quarters of cases respond to this. Those resistant to drugs, however, are offered surgical options:
- Radio frequency rhizotomy (RFR) is performed by first positioning the electrode correctly (see below), followed by lesioning at 10 ͒C increments from 50-90 ͒C ~ 1min. The electrode is adjusted intermittently to ensure that the lesioning covered the painful regions.
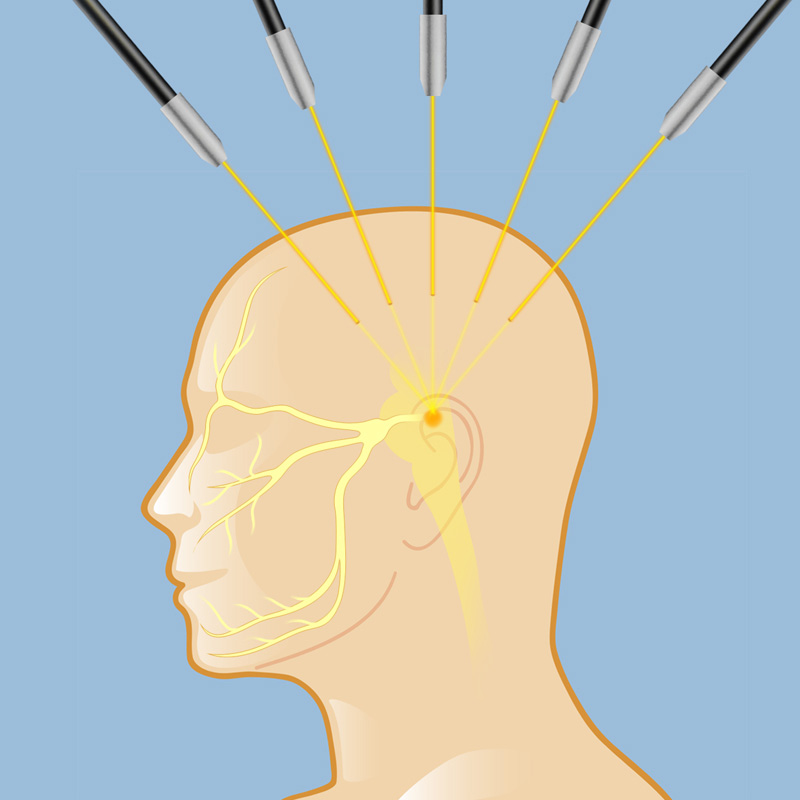
- Stereotactic radiosurgery (SRS) aka gamma knife/cyberknife is where radiation doses of 70-90 Gy is directed towards the root entry zone of the trigeminal nerve to lesion that region (see below).

{kind=link}
In MS TN is difficult to treat both pharmacologically and surgically. Holland et al. in this paper studied both their success rates (i.e. the likelihood of recurrence) and the costs of both surgically treatments in those who have failed medical treatment.
They report that at point of intervention their cases were on average on 2 medications for their TN. Both rhizotomy and radiosurgery provided good initial relief of pain symptoms. However, there was a higher rate of recurrence in those who underwent rhizotomy; requiring more procedures. Radiosurgery also has the added advantage of being minimally invasive and had a lower rate of complications. The rate of facial numbness is 60% and 66% for radiosurgery and rhizotomy, respectively. However, a disadvantage of the radiosurgery is the delayed onset of action taking anywhere between 1-6 weeks before it takes effect. Whereas, rhizotomy, initially had a higher risk of complication and discomfort, the pain relief was immediate. Radiosurgery was initially more expensive, but when you considered subsequent procedures the total cost was equivalent over time for both procedures.
Overall, these findings are very promising and both procedures should be made available to patients, particularly when taking into account the debilitating nature of trigeminal neuralgia and the side effects of medical treatments.
They report that at point of intervention their cases were on average on 2 medications for their TN. Both rhizotomy and radiosurgery provided good initial relief of pain symptoms. However, there was a higher rate of recurrence in those who underwent rhizotomy; requiring more procedures. Radiosurgery also has the added advantage of being minimally invasive and had a lower rate of complications. The rate of facial numbness is 60% and 66% for radiosurgery and rhizotomy, respectively. However, a disadvantage of the radiosurgery is the delayed onset of action taking anywhere between 1-6 weeks before it takes effect. Whereas, rhizotomy, initially had a higher risk of complication and discomfort, the pain relief was immediate. Radiosurgery was initially more expensive, but when you considered subsequent procedures the total cost was equivalent over time for both procedures.
Overall, these findings are very promising and both procedures should be made available to patients, particularly when taking into account the debilitating nature of trigeminal neuralgia and the side effects of medical treatments.