
Wunsch M, Jabari S, Voussen B, Enders M, Srinivasan S, Cossais F, Wedel T, Boettner M, Schwarz A, Weyer L, Göcer O, Schroeter M, Maeurer M, Woenckhaus M, Pollok K, Radbruch H, Klotz L, Scholz CJ, Nickel J, Friebe A, Addicks K, Ergün S, Lehmann PV, Kuerten S. The enteric nervous system is a potential autoimmune target in multiple sclerosis. Acta Neuropathol. 2017. doi: 10.1007/s00401-017-1742-6. [Epub ahead of print]
The opening line of the abstract gives a different twist usual science rag, it says that MS makes you poor. It gets weirder from there.
First we had the microbiota and the nervous system.
Did you spot the possible link between the microbiome and autoimmunity after alemtuzumab in our recent paper this week, yes there are hidden gems in there.
It is still free to download and read if you want click and follow the links.
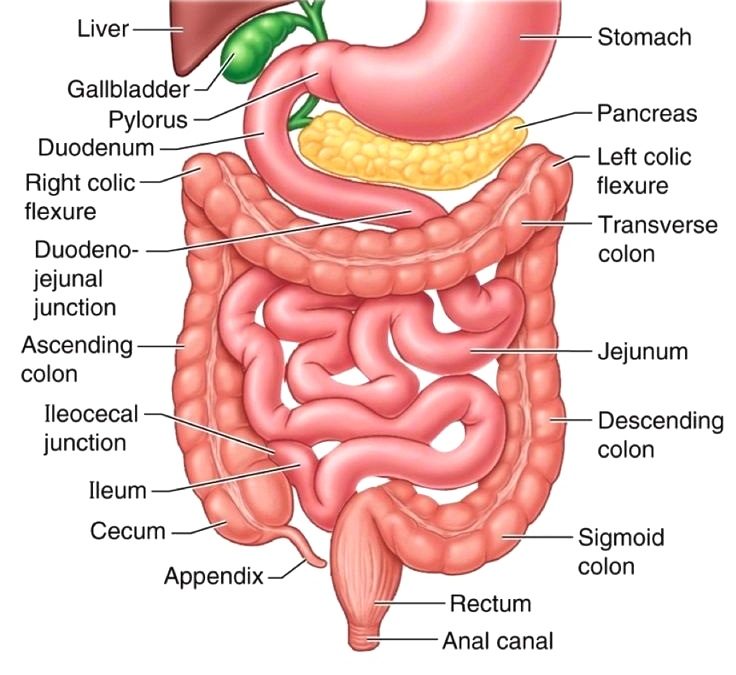
Now we are being told it is the enteric (gut) nervous system that's a problem. We would agree that with time that there are clearly problems with the gut in mice with EAE, and believe it or not we did a project looking at constipation, so in this case we can definitely say the chicken led to the egg. That the gut problems come after the autoimmunity of the CNS.
However, in this study they imply that the gut autoimmunity comes first. They report gut problems before there is evidence of autoimmunity in the CNS in an animal model. There was significantly less gut motility.
So should we make some students or MD2 count and weigh mouse poohs. It would not be surprising in mice with neurological EAE that there pooh count will be affected, as they eat and drink less when they are neurologically affected, but being a recipient of quite a few mouse number 2's in my time when holding a mouse, they maintain this function early in the disease course.
They found antibodies that targeted the gut in mice, which were present in some people with MS and there was some gut pathology with MS. If they had made the suggestion that MS was secondary to autoimmunity in lung tissue would this have been found?
But how does this disprove the possibility that lesions in the CNS has led to de-innervation of gut pathways and the effect is secondary to this. You are not going to get an answer against this from studying post-mortem MS years after disease onset.
But you are going to get support that there are gut changes in MS
Moser AM, et al. Mucosal biopsy shows immunologic changes of the colon in patients with early MS. Neurology, N2.
Objective: To investigate immune cells of the colonic mucosa and faecal short-chain fatty acids (SCFAs) in treatment-naive patients with a clinically isolated syndrome (CIS) or early relapsing MS.
Methods: In this cross-sectional proof-of-concept study, we obtained mucosal specimens during ileocolonoscopy from 15 untreated patients with CIS/MS and 10 controls. Mucosal immune cells were analyzed by FACS, and gas chromatography-mass spectrometry measurements of stool samples served to determine SCFA.
Results: The number of total dendritic cells (DCs), CD103+ tolerogenic DCs, and CD4+25+127–regulatory T cells (Tregs) was significantly reduced in the distal colon of patients with CIS/MS compared with controls, whereas we found no differences in the proximal colon. The patients' faecal samples also showed a substantially lower content of SCFA and especially lower levels of butyrate and acetate.
Conclusions: Our findings indicate a disturbed homeostasis of colonic DCs and Tregs in patients with MS which could be associated with colonic SCFA depletion. Although not implying causality, these findings confirm parallel abnormalities of the gut in MS and warrant further research if modulation of the colonic SCFA profile or the colonic Treg pool can serve to modify the course of MS.
But you are going to get support that there are gut changes in MS
Moser AM, et al. Mucosal biopsy shows immunologic changes of the colon in patients with early MS. Neurology, N2.
Objective: To investigate immune cells of the colonic mucosa and faecal short-chain fatty acids (SCFAs) in treatment-naive patients with a clinically isolated syndrome (CIS) or early relapsing MS.
Methods: In this cross-sectional proof-of-concept study, we obtained mucosal specimens during ileocolonoscopy from 15 untreated patients with CIS/MS and 10 controls. Mucosal immune cells were analyzed by FACS, and gas chromatography-mass spectrometry measurements of stool samples served to determine SCFA.
Results: The number of total dendritic cells (DCs), CD103+ tolerogenic DCs, and CD4+25+127–regulatory T cells (Tregs) was significantly reduced in the distal colon of patients with CIS/MS compared with controls, whereas we found no differences in the proximal colon. The patients' faecal samples also showed a substantially lower content of SCFA and especially lower levels of butyrate and acetate.
Conclusions: Our findings indicate a disturbed homeostasis of colonic DCs and Tregs in patients with MS which could be associated with colonic SCFA depletion. Although not implying causality, these findings confirm parallel abnormalities of the gut in MS and warrant further research if modulation of the colonic SCFA profile or the colonic Treg pool can serve to modify the course of MS.